Goals
- Understanding the molecular mechanisms underlying the bone effects of these drugs
- Understanding the genetic and molecular determinants of treatment response and tolerability
Results
- For this study I have primarily used the Framingham Heart Study (FHS) Osteoporosis ancillary study
- We have investigated the association between beta blocker use and higher bone density, and the dependence of this association on beta1-selectivity and dose, using a pharmacoepidemiologic study (1), where we have shown support for a protective effect of the drug both using propensity score analysis to minimize the influence of confounding variables, and through demonstration of a positive dose response
- Next, we discovered microRNA-mediated mechanisms of this clinical effect using supervised and unsupervised methods (2) in which we discovered that miR-19a-3p, previously found to be associated with beta blocker hypertensive response (3), was associated with higher bone density and beta blocker user in our study
- Finally, we conducted a pharmacogenomics study (4) in which we discovered and validated associations with beta-1 adrenergic receptor (ADRB1) and histone deacetylase 4 (HDAC4) in women. Interestingly, we showed an association between miR-19a-3p expression and the ADRB1 variant in the same direction as its association with bone density, supporting the targeting of beta-1 adrenergic receptor by miR-19a-3p to block adrenergic signaling and its negative impacts on bone.
Description of Molecular Hypotheses
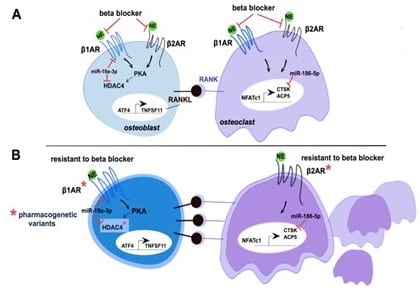
Figure 1: A. BBs target βARs in both osteoblasts and osteoclasts with hypothesized regulation by miRNAs. B.Pharmacogenetic variants (red stars)in b1AR and HDAC4 in osteoblasts and b2AR in osteoclastsdisrupt b1AR or b2AR binding to BBs or influence HDAC4 expression, causing osteoblast-mediated or direct changes in osteoclast differentiation and resorption.
Study Team
